
The response is built and waiting
Most patients given a checkpoint inhibitor do not respond. In a measurable subset the response is not absent but stalled, the T cells built and held in the lymph node. A frozen signature finds them across three cancers, and points to a lever and a test that needs no new patient.
Most patients given a checkpoint inhibitor do not respond. Close to half of cancer patients in the United States are now eligible for one of these drugs, and by one estimate about an eighth benefit (Haslam and Prasad, 2019). The rest are read as immunologically cold, and the field has no structural account of who they are or what, if anything, could be done for them.
For a measurable subset, the Garrison signature gives one. Their response is not absent. It is stalled. The tumour-specific T cells have been built and armed, and are held in the tumour-draining lymph node behind the egress step, while anti-PD-1 acts two positions downstream, at the synapse, where in these patients there is nothing yet to release. On a tumour biopsy a stalled response and an absent one read the same way, as a low T-cell count. They are not the same patient. A stalled response has a lever; an absent one does not.
What follows is the case that the state is real, that it can be measured across cancers, and that it is worth acting on.
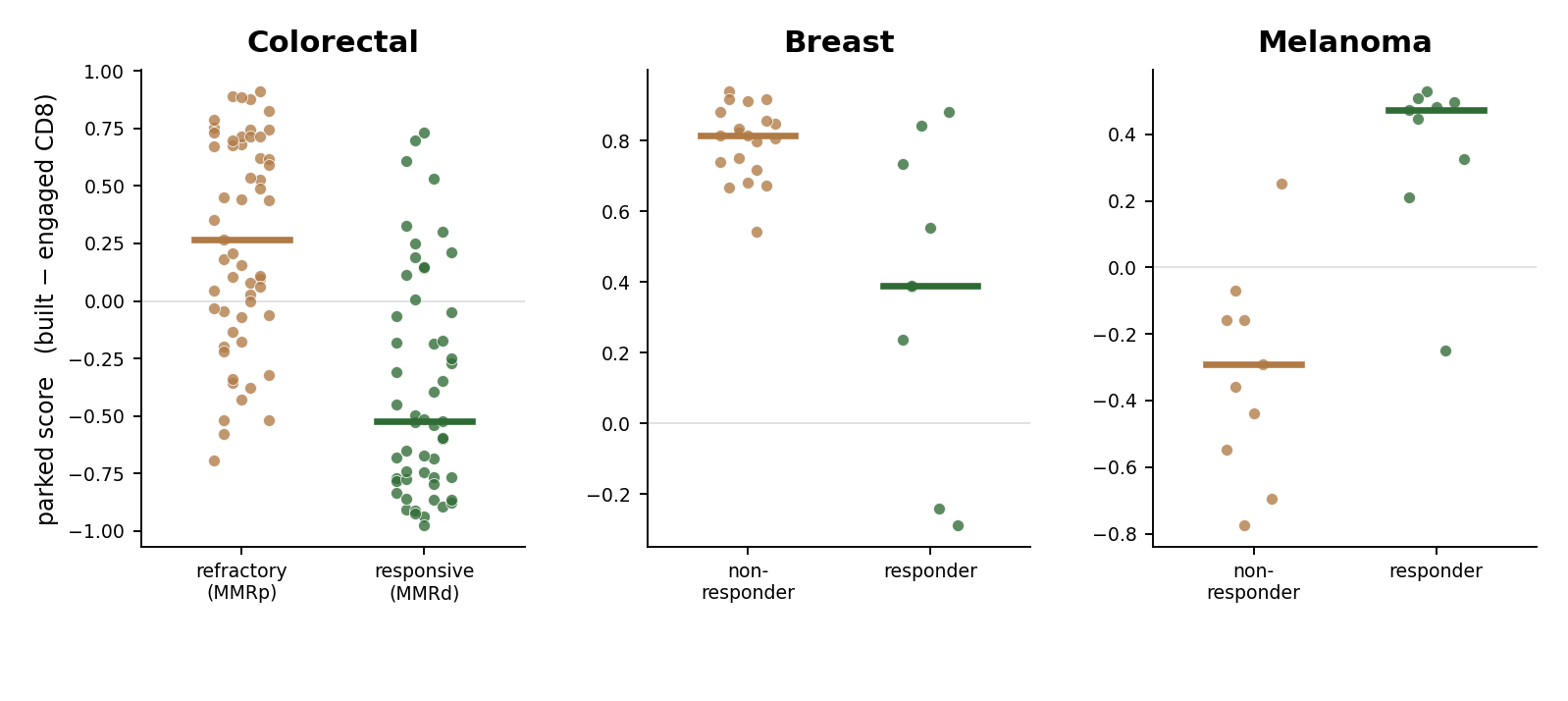
The signature holds across three cancers
The signature scores one quantity per sample: the built fraction of the CD8 compartment minus the engaged fraction. The thresholds are fixed before any data is opened, and no parameter is fit to outcome.
The entire analysis is public, and it runs in two seconds:
``` git clone https://github.com/raimovanderklein/garrison-signature cd garrison-signature && pip install scipy python garrison_scorer.py ```
The repository ships the per-sample data for all three cohorts and reproduces every number in this article. It is the whole argument, made checkable: github.com/raimovanderklein/garrison-signature.
| Cancer | Cohort | Response axis | n | Result |
|---|---|---|---|---|
| Colorectal | Pelka 2021 | MMR status | 110 biosamples | Garrison⁺ in refractory MMRp, Fisher **p = 0.0028** |
| Breast | Bassez 2021 | anti-PD-1 | 29 patients | parked → non-responder, **AUC 0.81** |
| Melanoma | Sade-Feldman 2018 | checkpoint | 19 patients | parked → **responder**, **AUC 0.94** (reversed) |
In colorectal and breast, the patients carrying a parked reserve are the ones in whom checkpoint blockade fails. The signature finds them from a single frozen definition, in two cancers, on public data.
The direction is predictable, which makes it portable
In melanoma the sign reverses: a parked reserve marks the responders. A signature that points one way in one cancer and the other way in another is not portable unless the direction can be set in advance. It can. Escobar et al. (2023) show that reliance on the stem-like reserve for checkpoint response depends on tumour immunogenicity: in a poorly immunogenic tumour the reserve is the limiting resource, so a reserve held back predicts failure, while in a highly immunogenic tumour effectors expand on their own and reserve abundance instead marks the responder. Colorectal and breast are low-immunogenicity, melanoma is high, and the observed sign matches the rule in all three. The melanoma cohort is read at baseline, before treatment, so the direction is a property of the cancer, not of the drug. The signature can therefore be applied to a new tumour type with its direction known beforehand, rather than fit after the fact.
Releasing it
If the response in these patients is built and held back, the intervention is to release it. CD40 agonism supplies the licensing signal the parked cell is waiting for. CD40 agonist antibodies are already in the clinic, sotigalimab and selicrelumab among them, with activity that has been real and uneven. The uneven part reads as a selection problem: the agonist should help the parked patient and do little for the rest, and a trial that enrols both without stratifying averages them into a muted result.
That is testable on samples that already exist. CD40 agonists have been given alongside checkpoint inhibitors, and the baseline biopsies from those trials sit in freezers. Score them for the signature and ask one question: did the benefit of adding the agonist concentrate in the signature-positive patients? A muted trial result becomes a stratified subgroup analysis, with no new patient enrolled and no new drug given. That re-analysis is what a prospective, signature-selected arm would have to earn first.
Limits
The signature is locked at single-cell resolution. The version that reads the same state in an ordinary bulk or fixed biopsy, the kind held in trial freezers, still has to be built and validated, and it is that version the retrospective test depends on. The melanoma cohort is scored from marker genes rather than annotated cell types, a coarser method than the cell-fraction scoring used in colorectal and breast. And the direction rule is taken from Escobar et al.; deriving it from the framework's own primitives is unfinished.
The non-responders are treated as the patients immunotherapy has nothing left to offer. For the subset whose response is built and waiting, the question is not whether they mounted one, but whether it can be released.
The signature, defined: The Garrison Signature (van der Klein, 2026), 10.5281/zenodo.20479100. The cycle it sits on: Completing the Chen-Mellman cancer-immunity cycle. The code: github.com/raimovanderklein/garrison-signature.